Epilepsy Research
Epilepsy is a neurological disorder in which brain activity becomes abnormal, causing seizures or periods of unusual behavior, sensations, and sometimes loss of awareness. The brain's abnormal activity could be due to an inherited genetic condition, trauma diseases or developmental disorders of the brain. Epilepsy is one of the most common chronic neurologic conditions affecting 0.5-1% children. Antiseizure medications are the first choice of treatment for epilepsy, however, they have side effects and cannot control the seizures in approximately 30% of patients. For these patients, the most promising treatment is brain surgery. Epilepsy surgery has advanced significantly, and nowadays good results can be expected in approximately half of the patients. Epilepsy surgery should be performed early in life to allow the still growing and developing pediatric brain to recover normal brain functions after surgery.
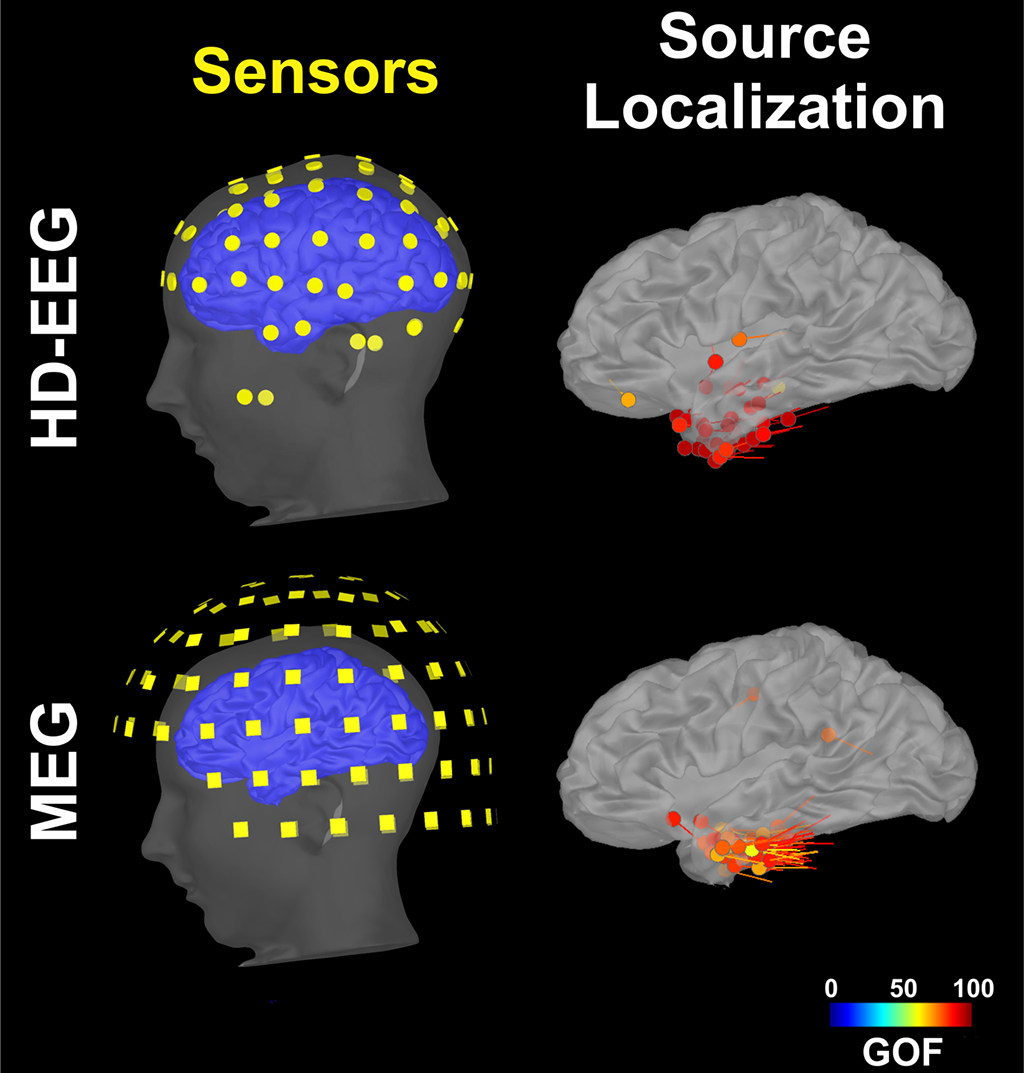
The goal of epilepsy surgery is the resection of the brain area which is essential for the generation of seizures. This area is called the epileptogenic zone (Fig. 1). Complete resection of this area may lead to medication and seizure freedom. Yet, this area is theoretical, meaning that there is no tool or method to directly identify it with precision. To define the epileptogenic zone, children who are good candidates for epilepsy surgery undergo an extensive presurgical evaluation which involves several tests that help to pinpoint other brain areas which are indirect estimates of the epileptogenic zone. For example, these tests can identify the brain area that generates abnormal electrical signals (i.e. epileptic spikes), called irritative onset zone, or the brain area where the seizures begin, the so-called ictal (or seizure) onset zone (Fig. 1). Magnetoencephalography (MEG) and high-density electroencephalography (HD-EEG) are two of these tests that are able to detect and localize spikes, which are epileptic activity generated by the irritative zone (Fig. 2). The irritative zone defined by these tests is a good approximate estimator of the epileptogenic zone (Fig. 3). These tests also help to precisely identify important areas in the brain which are responsible for the different normal functions, for example movements and speech. These areas are called eloquent areas (Fig. 1) and should not be resected during surgery in order to avoid functional deficits.
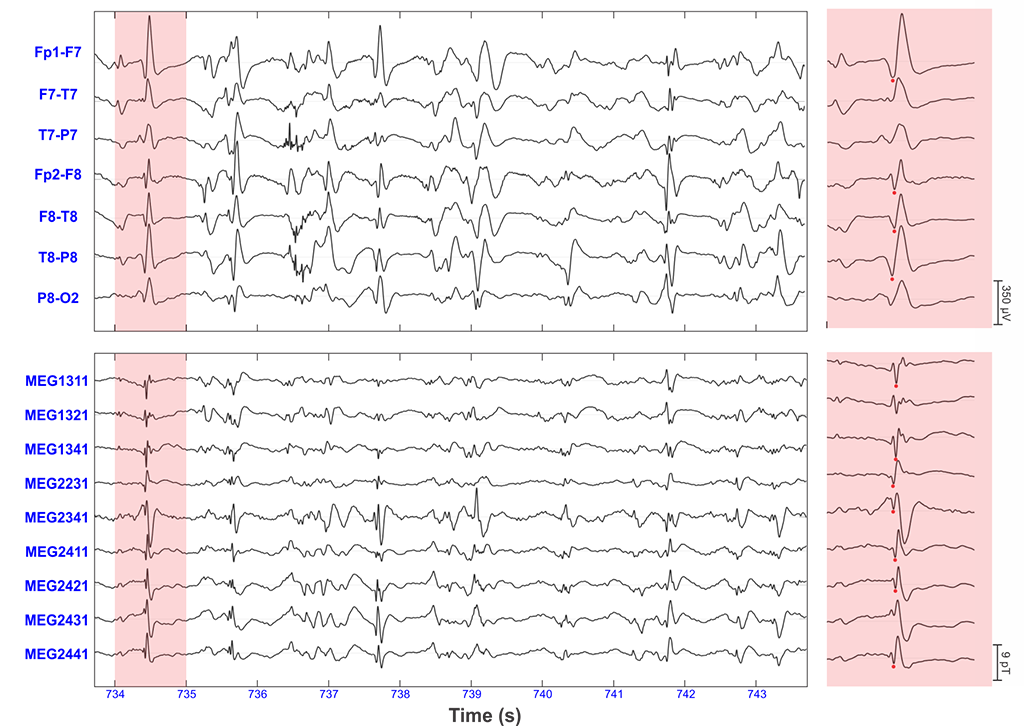
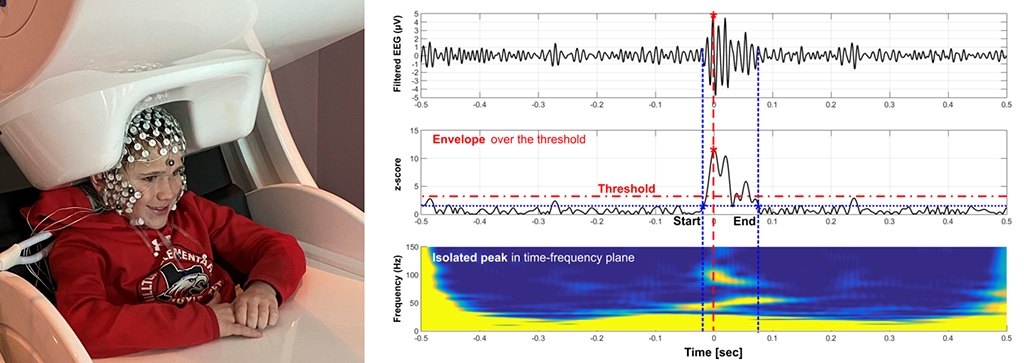
Yet, the results of these tests are sometimes inconclusive or contradictory. Thus, new techniques and data analysis methods need to be developed in order to help reliably identify the epileptogenic zone. Funded by the National Institute of Neurological Disorders and Stroke, our research team led by Dr. Christos Papadelis (Principal Investigator) works closely with our epilepsy medical team at Cook Children’s Health Care System (Dr. Scott Perry and his team) and collaborators at Boston Children’s Hospital (Dr. Phillip Pearl and his team) and Massachusetts General Hospital (Dr. Steven Stufflebeam and his team) to develop such new biomarkers. The team focuses its efforts on signals which seem to be generated particularly by the epileptogenic zone. These signals are called high frequency oscillations (or HFOs) and are characterized by fast oscillatory activity in the frequency range between 80 and 500 Hz. HFOs can be recorded using invasive techniques such as stereotaxic electroencephalography (sEEG), but our group has shown strong evidence that HFOs can also be recorded non-invasively using scalp electroencephalography (EEG) or magnetoencephalography (MEG) (Fig. 4 - left) (see Papadelis et al., 2016; Tamilia et al., 2017; Tamilia et al., 2020). Figure 4 (right panel) shows an example of an HFO detected non-invasively with EEG and MEG. The development of such a non-invasive biomarker of epilepsy would augment the presurgical evaluation of children with refractory epilepsy by guiding the placement and implantation of intracranial EEG and facilitate the surgical planning for these patients.
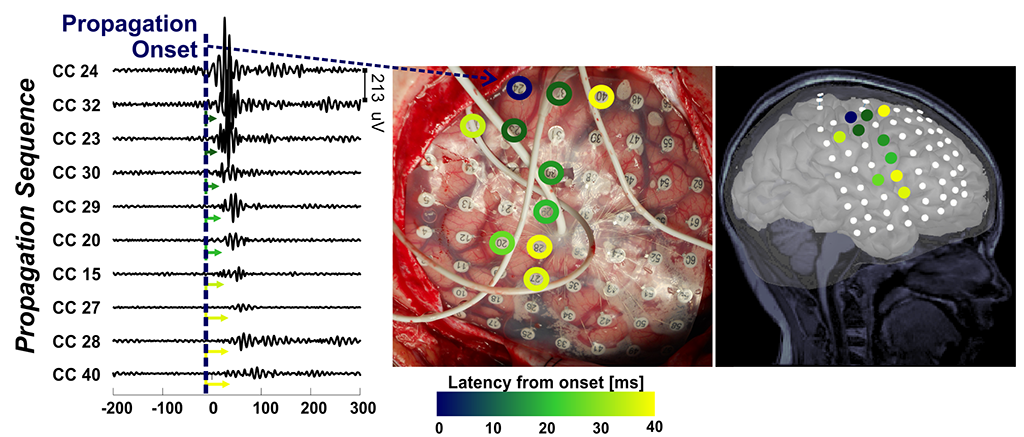
One challenge that our team faces is that HFOs are generated in large areas of the brain which often overlap with the eloquent brain areas that should not be resected during epilepsy surgery. On intracranial recordings, we have showed that the HFOs propagate across several areas of the brain and that the onset of this propagation is a promising specific biomarker to the epileptogenic zone (Fig. 5). Thus, there is no need to surgically resect all the area that generates the HFOs; surgical resection of the onset generator is sufficient in order for the child to, hopefully, become seizure free.
Selected publications
C Papadelis, E Tamilia, S Stufflebeam, PE Grant, JR Madsen, PL Pearl, N. Tanaka. Interictal high frequency oscillations detected with simultaneous magnetoencephalography and electroencephalography as biomarker of pediatric epilepsy. JoVE (Journal of Visualized Experiments) 2016, e54883.
E Tamilia, JR Madsen, PE Grant, PL Pearl, C Papadelis. Current and emerging potential of magnetoencephalography in the detection and localization of high-frequency oscillations in epilepsy. Frontiers in Neurology 2017; 8, 14.
E Tamilia, M AlHilani, N Tanaka, M Tsuboyama, JM Peters, PE Grant, Madsen JR, Stufflebeam SM, Pearl PL, Papadelis C. Assessing the localization accuracy and clinical utility of electric and magnetic source imaging in children with epilepsy. Clinical Neurophysiology 2019; 130 (4), 491-504.
C Papadelis, YH Chen. Pediatric Magnetoencephalography in Clinical Practice and Research. Neuroimaging Clinics 2020; 30 (2), 239-248.
E Tamilia, M Dirodi, M Alhilani, PE Grant, JR Madsen, SM Stufflebeam, Pearl PL, Papadelis C. Scalp ripples as prognostic biomarkers of epileptogenicity in pediatric surgery. Annals of Clinical and Translational Neurology 2020; 7 (3), 329-342.
E Tamilia, EH Park, S Percivati, J Bolton, F Taffoni, JM Peters, PE Grant, Pearl PL, Madsen JR, Papadelis C. Surgical resection of ripple onset predicts outcome in pediatric epilepsy. Annals of neurology 2018; 84 (3), 331-346.